My child needs their adenoids and tonsils removed and palate expansion – what should we do first?
Many snoring children will have immediate sleep and symptomatic improvements with surgical removal of enlarged adenoids and tonsils.
However, research tells us surgery is not a complete cure. Often children will have residual breathing disturbances during sleep, or a recurrence of symptoms with time.
This is because snoring and other disturbed breathing is a multifactorial problem and there are usually a combination of risk factors that contribute to the issue, and need to be addressed.
In fact, there is growing support for the hypothesis that enlarged adenoids and tonsils may be a symptom of a greater underlying airway problem, including poor palate development, nasal disuse and dysfunctional breathing during sleep.
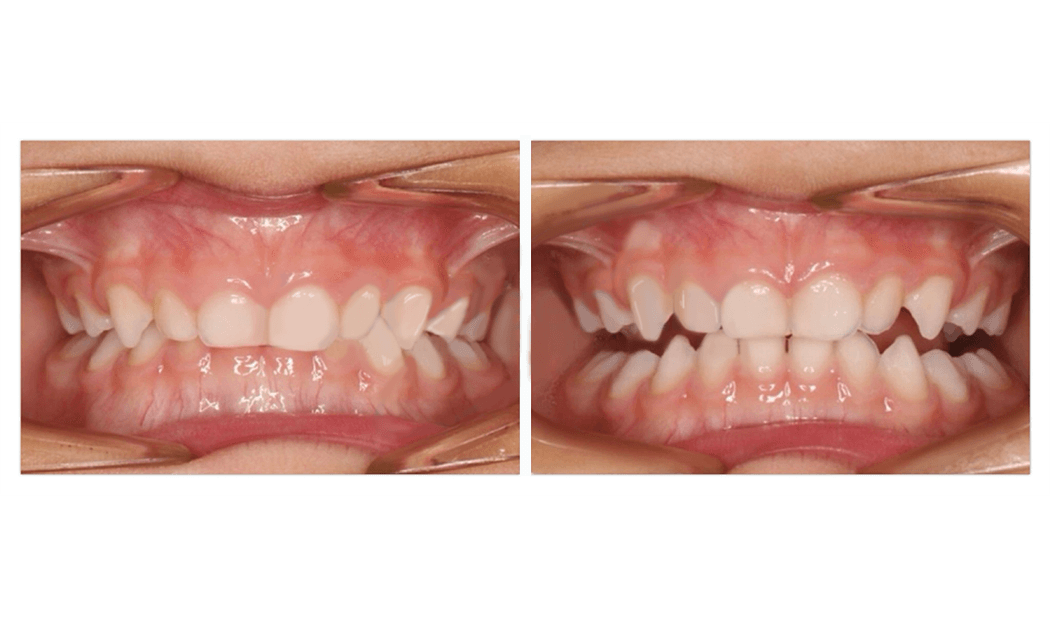
Palate expansion
- Is well proven as an adjunct to removal of adenoids and tonsils to address snoring and obstructive sleep apnoea
- Has been well demonstrated to help improve nasal airflow and nasal breathing
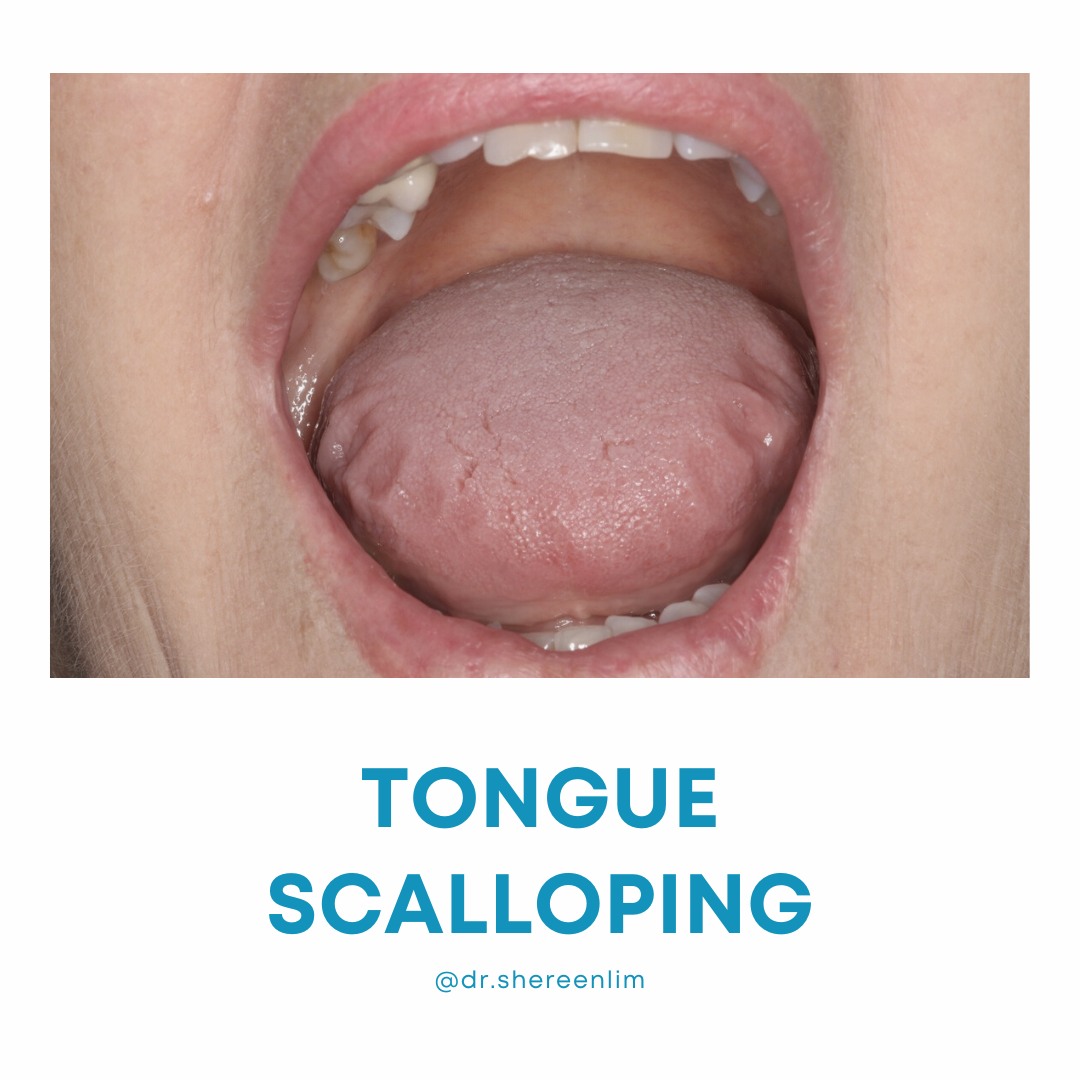
- Improves tongue space. This can promote or facilitate better tongue to palate seal and less encroachment of the base of tongue in the throat.
- Has been demonstrated to reduce the volume of the adenoids and tonsils, and improve symptoms of disturbed sleep in one study published this year https://europepmc.org/article/pmc/pmc9213408
When a child has a constricted palate, a common question is what should we address first?
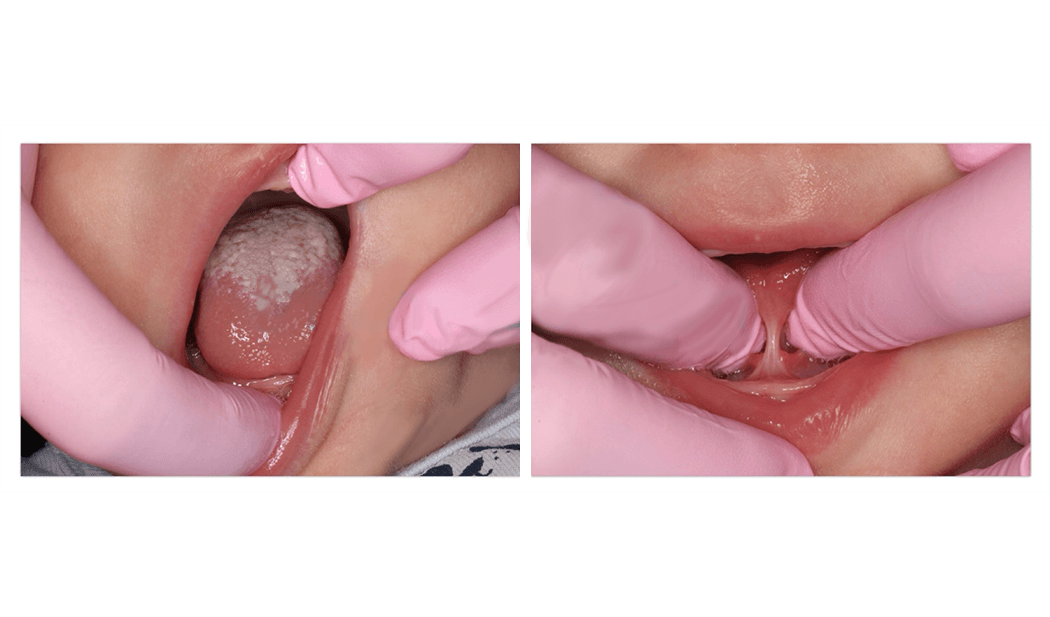
If a child is too young to engage directly with us and sit in the chair for a full series of orthodontic photos, then palate expansion is not an option. Surgery first to remove enlarged adenoids and tonsils can be a good option to help open the airway. This is because young children are most vulnerable to unrestorative sleep, and increased risks of behavioural and learning problems down the track.
From around 3 years, some children will be ready to engage directly with us, and co-operate for a complete series of orthodontic photos. These children may be good candidates to start palate expansion.
Often it can take time to get an ENT consult or a date for surgery, so it’s common for me to suggest we start expansion prior.
In fact sometimes children are recommended surgery based on symptoms, and without a proper assessment using a video endoscope of the nose and throat. Apart from certain x-rays, this is the only way to visualize for certain that the adenoids are in fact obstructing the airway. I would rather address narrow palate, or what we know for certain is there and contributing to limitation of airflow, and reassess response to expansion over the first 4-6 weeks.
One of the benefits with this approach is that if breathing, sleep and day function is improving quickly within that time frame, then it could be an indication that a child may be able to avoid surgery.
This is something I see often, but individual results will vary depending on each child’s combination of risk factors.
To make the most fully informed decision on what is right for your child, it is best to have an individualised assessment, and a second opinion from your ENT surgeon.